Surgery, Treatments and Therapies
There are a wide array of treatment options for someone suffering through Parkinson's, yet none of these offer a permanent solution to this disease. This is why continued research is essential to finding a cure. All of these treatments are symptomatic therapies, meaning that they are techniques designed to reduce motor and non-motor symptoms, delay the continuous growth of the disease and also to decrease the side effect of the medications. Below is an extensive list of the latest research in Parkinson's Disease treatment.
Levodopa
“Levodopa remains the most effective agent to improve motor symptoms in PD but, as noted earlier, chronic use is associated with the emergence of motor fluctuations. This is manifested by a loss of clinical benefit before the next levodopa dose (wearing off), dyskinesias (abnormal involuntary movements), and nonmotor complications, such as behavioral and cognitive changes” (Tambasco et al., 2012).
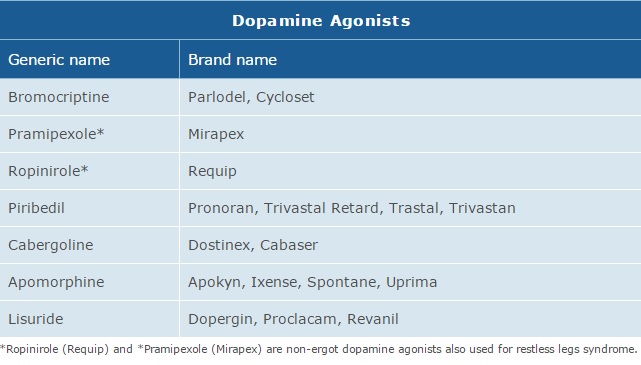
Dopamine Agonists
“Dopamine agonists are molecules that bind to the postsynaptic dopamine receptors and mimic the role of dopamine in the brain, causing a response similar to dopamine itself. Agonists were initially used to alleviate symptoms during the “off” state in patients with late PD when the benefits of levodopa doses were wearing off. Agonists are also used as an early alternative to levodopa so that later complications and dyskinesias are postponed for as long as possible”(Robertson. A Train Education: Continuing Education for Health Professionals).
There are a wide array of treatment options for someone suffering through Parkinson's, yet none of these offer a permanent solution to this disease. This is why continued research is essential to finding a cure. All of these treatments are symptomatic therapies, meaning that they are techniques designed to reduce motor and non-motor symptoms, delay the continuous growth of the disease and also to decrease the side effect of the medications. Below is an extensive list of the latest research in Parkinson's Disease treatment.
Levodopa
“Levodopa remains the most effective agent to improve motor symptoms in PD but, as noted earlier, chronic use is associated with the emergence of motor fluctuations. This is manifested by a loss of clinical benefit before the next levodopa dose (wearing off), dyskinesias (abnormal involuntary movements), and nonmotor complications, such as behavioral and cognitive changes” (Tambasco et al., 2012).
Dopamine Agonists
“Dopamine agonists are molecules that bind to the postsynaptic dopamine receptors and mimic the role of dopamine in the brain, causing a response similar to dopamine itself. Agonists were initially used to alleviate symptoms during the “off” state in patients with late PD when the benefits of levodopa doses were wearing off. Agonists are also used as an early alternative to levodopa so that later complications and dyskinesias are postponed for as long as possible”(Robertson. A Train Education: Continuing Education for Health Professionals).
MAO-B Inhibitors
“Selegiline (Eldepryl, Deprenyl, or Selgene) and rasagiline (Azilect) are MAO-B inhibitors that increase the level of dopamine in basal ganglia synapses by blocking its metabolism. They inhibit the monoamine oxidase-B (MAO-B) enzyme responsible for breaking down dopamine. Like dopamine agonists, MAO-B inhibitors alone can improve motor symptoms and delay the need for levodopa early in the disease, but they are less effective than levodopa. In the advanced disease, they can be used to reduce fluctuations between “on” and “off” periods. None of these treatments slow the progression of the disease”(Robertson. A Train: Continuing Education for Health Professionals).
Transdermal Patches and Intestinal Gels
“Duodopa requires an attentive caregiver who must manage the device, the skin surrounding the tube, and medication refills. Early studies have revealed high rates of device-related problems with the intestinal tube (eg, clogging, kinking, moving out of the correct location). Despite these tube-related issues, Duodopa will likely be a great choice for many patients with on-off fluctuations, and will in most cases allow discontinuation of oral PD drugs” (Okun, 2012).
“Selegiline (Eldepryl, Deprenyl, or Selgene) and rasagiline (Azilect) are MAO-B inhibitors that increase the level of dopamine in basal ganglia synapses by blocking its metabolism. They inhibit the monoamine oxidase-B (MAO-B) enzyme responsible for breaking down dopamine. Like dopamine agonists, MAO-B inhibitors alone can improve motor symptoms and delay the need for levodopa early in the disease, but they are less effective than levodopa. In the advanced disease, they can be used to reduce fluctuations between “on” and “off” periods. None of these treatments slow the progression of the disease”(Robertson. A Train: Continuing Education for Health Professionals).
Transdermal Patches and Intestinal Gels
“Duodopa requires an attentive caregiver who must manage the device, the skin surrounding the tube, and medication refills. Early studies have revealed high rates of device-related problems with the intestinal tube (eg, clogging, kinking, moving out of the correct location). Despite these tube-related issues, Duodopa will likely be a great choice for many patients with on-off fluctuations, and will in most cases allow discontinuation of oral PD drugs” (Okun, 2012).
Deep Brain Stimulation
“Deep brain stimulation is a surgical intervention that utilizes an implantable pulse generator (neurostimulator) as a waveform generator and power source. The neurostimulator controls the flow of current to specific brain regions through an attachment to an implantable DBS lead. Each DBS lead has multiple contacts and therefore many possible parameter configurations. The optimization of possible settings, which may number into the thousands when considering the range of pulse widths, frequencies, amplitudes, and configuration of anodes and cathodes, can provide a critical determinant for therapeutic success or failure” (Fakhar et al., 2013).
For the procedure a device called a implantable pulse generator (IPG) is placed, which effectively blocks abnormal nerve signals via electrical stimulation. As of now, the procedure is only for patients whose symptoms are unable to be controlled by medication and other means. This is only a temporary solution to the side effects of PD and this is by no means a cure. The IPG merely blocks and regulates abnormal electrical signals. Fortunately if newer treatments prove more effective or Deep Brain Stimulation ends up causing side effects, the IPG can be removed or adjusted.
A Personal Story:
Deep Brain Stimulation is an option for patients with severe Parkinson’s. In this procedure wiring is essentially installed into brain in order to generate electric impulses deep inside the brain tissue. A battery pack is then placed near the heart to power the device.The technique for this procedure is obviously very risky because there is the extreme risk that permanent damage can be done to blood vessels during surgery when the doctors are inserting the electrodes into the brain. The chance of infection is also a considerably high risk.
A patient by the name of Alan underwent this very procedure. He talks about his experience,
“My surgeries were scheduled for August 2011. There were three in all. The first two were to open holes in my skull and put the wiring in place and the third was to install the device that creates the electrical impulse and connects everything together.During the first two surgeries I was conscious. My skull was placed in a halo device to hold it steady. During the surgery the neurologist asked me to do certain movements at his command.Someone asked me how it was to be conscious while the procedure was going on. I said that the hard part was hearing the drill as it bore through my skull.”
(Robertson. A Train Education: Continuing Education for Health Professionals).

Genetic Testing
“Genetic testing is the advanced technique used to analyze human DNA, RNA, and proteins in order to detect specific disease or condition. Genetic testing has recently become available for the Parkin and PINK1 genes. But because Parkin is such a large gene, testing is difficult. At the current stage of understanding, testing is likely to give a meaningful result only for people who develop the condition before the age of 30 years” (NHGRI, 2011).
“Gene therapy is “the use of genes as medicine” involving the transfer of a therapeutic or working copy of a gene into specific cells in order to repair a faulty gene or to give the cell a new function” (Centre for Genetics Education, 2012).
Neurturin Gene Therapy
“A third gene therapy technique using neurturin hopes to “rescue” sick dopaminergic nerve cells by injecting a growth/trophic factor. The goal is to help damaged nerve cells repair themselves. In this gene therapy study, the viral genes were removed and the genes to make neurturin were inserted. The altered virus was then injected into the brains of study participants. The phase 1 study involved 12 patients who were followed for 1 year. Over the course of a year their UPDRS showed significant improvement. Although the phase 1 trial seemed to improve the patient’s symptoms, researchers were unable to replicate the positive results in a larger, phase 2 study (Aminoff, 2010).
ProSavin Gene Therapy
ProSavin is a Parkinson’s therapy designed to combine the genes of the three essential enzymes in dopamine production. The therapy involves inserting a large quantity of these essential genes into the basal ganglia region of the brain, coaxing the cells into a continuous dopamine supply. The results of recent clinical studies showed improved motor behavior in most all patients with no serious adverse effects.
“Genetic testing is the advanced technique used to analyze human DNA, RNA, and proteins in order to detect specific disease or condition. Genetic testing has recently become available for the Parkin and PINK1 genes. But because Parkin is such a large gene, testing is difficult. At the current stage of understanding, testing is likely to give a meaningful result only for people who develop the condition before the age of 30 years” (NHGRI, 2011).
“Gene therapy is “the use of genes as medicine” involving the transfer of a therapeutic or working copy of a gene into specific cells in order to repair a faulty gene or to give the cell a new function” (Centre for Genetics Education, 2012).
Neurturin Gene Therapy
“A third gene therapy technique using neurturin hopes to “rescue” sick dopaminergic nerve cells by injecting a growth/trophic factor. The goal is to help damaged nerve cells repair themselves. In this gene therapy study, the viral genes were removed and the genes to make neurturin were inserted. The altered virus was then injected into the brains of study participants. The phase 1 study involved 12 patients who were followed for 1 year. Over the course of a year their UPDRS showed significant improvement. Although the phase 1 trial seemed to improve the patient’s symptoms, researchers were unable to replicate the positive results in a larger, phase 2 study (Aminoff, 2010).
ProSavin Gene Therapy
ProSavin is a Parkinson’s therapy designed to combine the genes of the three essential enzymes in dopamine production. The therapy involves inserting a large quantity of these essential genes into the basal ganglia region of the brain, coaxing the cells into a continuous dopamine supply. The results of recent clinical studies showed improved motor behavior in most all patients with no serious adverse effects.
Transcranial Sonography
“The search for a cheap and patient-friendly technique to diagnose PD has continued, and over the past ten years transcranial sonography of the substantia nigra has emerged as a promising tool. Numerous ultrasound studies have found that a significant percentage of patients with idiopathic PD have a typical enlarged area in the substantia nigra, which is thought to be associated with increased iron concentrations” (Boewmans, 2013).
Neuroprotective Therapy
Neuroprotective therapy is a procedure that theoretically aims to slowdown the progression of Parkinson’s Disease. It is based around the concept that “the three to four hundred thousand at-risk dopaminergic neurons in the human substantia nigra can somehow be protected from the complex degenerative process that causes premature cell death and depletion of dopamine.” (Tarsy, 2014).
Neural Transplantation
Neural transplantation is an approach to the treatment of neurodegenerative diseases such as PD by replacing lost neurons, namely dopaminergic neurons. Early clinical trials have successfully shown that ”that human fetal dopaminergic neurons can survive and function for more than 10 years in the striatum of patients with PD and show no signs of being affected by the ongoing disease process.”(Bjorklund, June 2003) The biggest problem with these trials remains to be the inconsistency of them. This further outlines how we both do not fully understand how to optimally address target areas, as well as our limited understanding of the disease.
“The search for a cheap and patient-friendly technique to diagnose PD has continued, and over the past ten years transcranial sonography of the substantia nigra has emerged as a promising tool. Numerous ultrasound studies have found that a significant percentage of patients with idiopathic PD have a typical enlarged area in the substantia nigra, which is thought to be associated with increased iron concentrations” (Boewmans, 2013).
Neuroprotective Therapy
Neuroprotective therapy is a procedure that theoretically aims to slowdown the progression of Parkinson’s Disease. It is based around the concept that “the three to four hundred thousand at-risk dopaminergic neurons in the human substantia nigra can somehow be protected from the complex degenerative process that causes premature cell death and depletion of dopamine.” (Tarsy, 2014).
Neural Transplantation
Neural transplantation is an approach to the treatment of neurodegenerative diseases such as PD by replacing lost neurons, namely dopaminergic neurons. Early clinical trials have successfully shown that ”that human fetal dopaminergic neurons can survive and function for more than 10 years in the striatum of patients with PD and show no signs of being affected by the ongoing disease process.”(Bjorklund, June 2003) The biggest problem with these trials remains to be the inconsistency of them. This further outlines how we both do not fully understand how to optimally address target areas, as well as our limited understanding of the disease.

Embryonic Stem Cells
“Dopaminergic neurons can be generated from stem cells of different sources.Embryonic stem cells (ESCs) have unlimited self-renewal capacity and are pluripotent, since they are able to generate cells of all three germ layers. Somatic(tissue-derived) stem cells can be isolated from developing tissues of the fetus or in the newborn, juvenile, or adult organism. Somatic stem cells have a more limited proliferation capacity than ESCs and are termed multipotent, typically being able to differentiate into the different cell types of one germ layer. Potential groups of stem cells for PD cell therapy include embryonic stem cells, neural stem cells, mesenchymal stem cells, and, more recently, induced pluripotent stem cells” (Jensen et al., 2011).
The emphasis of stem cell research is finding ways to replace damages or dead cells. Researchers suggest this may affect PD by replacing/creating both nerve cells and dopamine-producing cells. Animal trials for this research are already well underway and now focused on safer, reliable treatment for humans, as human trials should begin in the coming years.
